It is without question that, when used correctly and with recommended operating parameters to maximize laser-tissue interaction, laser-assisted surgical procedures on soft and hard tissue are less physically injurious when compared to both scalpel and electrosurgery. Patient acceptance, peer pressure and a general acceptance of "hi-tech" approach to treatment may all propose an enhancement of tolerance of sensory stimulation.
Lasers can help you provide a higher level of care. In restorative dental procedures, management of soft tissue is simplified because the tedious and painful placement of retraction cord can be eliminated. Better impressions are possible for indirect restorations such as crowns and bridges, and clearer margins near the gingiva are revealed for optical scanning. Class V carious lesions can be prepared at or near the subgingival level with excellent hemostasis. This ensures an improved bond for composite materials and ultimately results in better aesthetics and a longer-lasting restoration. Two minutes of disinfection treatment of an aphthous ulcer brings immediate relief to the patient who may have been suffering for days. Excellent hemostasis can be achieved during minor surgical procedures like an immediate loading implant or second-stage implant uncovering. Not only is there a clean dry operating site, but the improved visualization will save time for the other steps of the treatment. All this will save your time.
1. Difference in Pulp Therapy and Pulpotomy
Pulpotomy techniques for primary teeth traditionally have used formocresol, but this is becoming less widely used because of its toxic effects on living tissues and mutagenic potential. Alternatives such as MTA are expensive, and this has led to interest in using lasers for pulpotomy procedures. The lasers used have included diode lasers, Nd:YAG, and Er:YAG laser. Several clinical studies support the use of lasers for pulpotomy. The reported advantages include better clinical as well as radiographic outcomes than ferric sulphate, MTA or electrosurgery, as well as a shorter operating time, simpler procedure and less postoperative pain. Effective photothermal disinfection combined with low-level laser effects likely accounts for the favorable outcomes seen clinically with laser pulpotomy. Similarly, there is clinical trial data to support the effectiveness of direct pulp capping using lasers with diode diode, Er:YAG and Er,Cr:YSGG lasers.
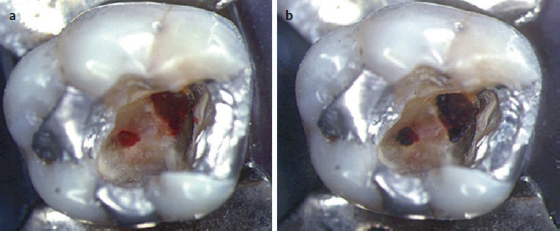 Left: Bleeding pulp at the base of the cavity preparation following an iatrogenic exposure of vital pulp tissue. Right: Immediately after firing several pulses of carbon dioxide laser radiation to seal the area and control bleeding. The cavity was then lined with glass ionomer cement and the tooth restored with amalgam. There was no loss of vitality over time.
Left: Bleeding pulp at the base of the cavity preparation following an iatrogenic exposure of vital pulp tissue. Right: Immediately after firing several pulses of carbon dioxide laser radiation to seal the area and control bleeding. The cavity was then lined with glass ionomer cement and the tooth restored with amalgam. There was no loss of vitality over time.
2. Difference in Troughing Prior to Impression
In implant dentistry, the margin of the abutment may be subgingival in some instances. To prepare the gingival tissues for an accurate impression for the final restoration, a “sulcus” or space must be created; and the procedure is often referred to as troughing.
For non-implant restorative procedures, this is accomplished with retraction cords, the scalpel, or electrosurgery. Electrosurgery is contraindicated around implants, but retraction cord or a scalpel is an option. However, the retraction cord technique is time-consuming with potential to injure the gingiva as well as to cause postoperative discomfort. Use of a scalpel may result in reduction in the width of attached gingival postoperatively and also some amount of postoperative discomfort. In contrast to conventional techniques, laser troughing allows for clear clean visualization of gingival margins. Most lasers are excellent coagulation devices with minimal to no bleeding. Lasers usually require 30-60 s to achieve retraction which does not rebound because lasers remove the internal epithelial lining of the gingival sulcus. Also another advantage of laser troughing is that it promotes the ideal environment for current impression scanning devices. All of the currently available wavelengths can perform this procedure.
 Left: A diode laser is used for troughing delivered through a 200-diameter micron tip. Right: 1 week postoperative healing
Left: A diode laser is used for troughing delivered through a 200-diameter micron tip. Right: 1 week postoperative healing
3. Difference in Soft Tissue Procedures
The healthy gingival margin is located 1-2 mm coronal to the cemento-enamel junction. However, this gingival architecture does not always present smile aesthetics during or after orthodontic treatment. Mucogingival surgery on the other hand, is a periodontal treatment to correct the defects in the morphology, position and/or amount of soft tissue and underlying bone support around teeth and implants.
Laser incision/excision definitely has a place in modern mucogingival surgery. Compared with a scalpel, a laser beam or the initiated fiberoptic tip of laser device can more easily cut, ablate and reshape the oral soft tissues in the oral cavity, with no or reduced bleeding and less pain, as well as with no or less need for suturing. This represents a range of tissue interactions, such as tissue warming, welding, coagulation, protein denaturation, drying and finally vaporisation (ablation) and carbonisation, where soft tissues are evaporated or incised. This process also provides haemostasis, microbial inhibition and destruction and photobiomodulation (PBM).
In particular, there is increasing evidence that the appropriate use of lasers is associated with reduced intraoperative and post-operative pain and enhanced wound healing or tissue regeneration, compared to conventional use of scalpel or electrosurgery. Electrosurgery can be used for incising soft tissues with good haemostasis, but comes with a risk of delayed wound healing due to unwanted thermal damage and necrosis of the underlying periosteum and alveolar bone.
4. Difference in Gingival and Lip Pigmentation Management
A well-aligned set of teeth not only improves function and oral hygiene maintenance but most importantly produces a confident and attractive smile. Gingival contour, emergence profile, and teeth proportion all contribute to the smile profile. However, dark pigmentation of the gingiva and lip may deflect the attention of a perfect smile.
The use of chemical peel and cryosurgery has been used for melanin depigmentation. Treatment with scalpel and diamond bur has also been used and compared with lasers. In a split-mouth clinical trial, the use of lasers has been shown with less relapse 3 months post-op when compared with electrosurgery.
Previous:Debridement of the Root Canal System by Diode Laser
Next:No content